Gall Bladder Duplication
A Rare Anomaly Detected on Preoperative Imaging
Hellenic Journal of Surgery on 27 October 2015
Abstract
Case History
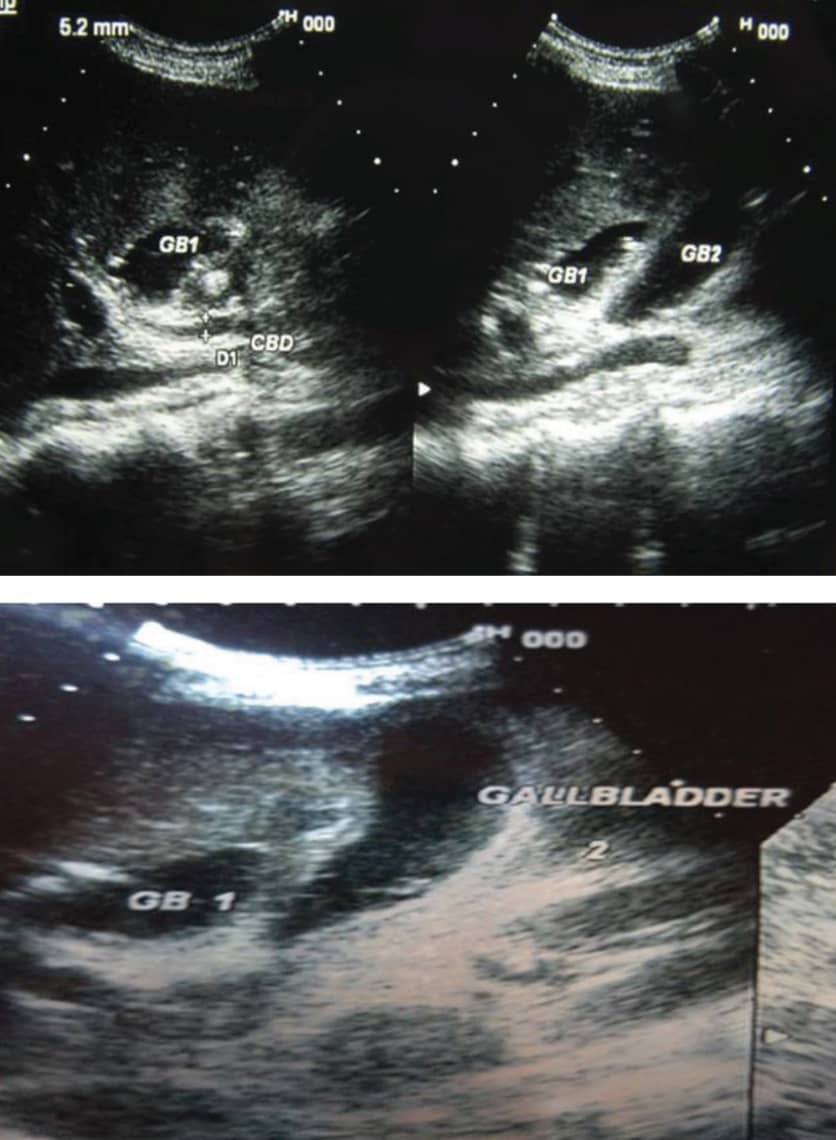
USG showing duplication of the gallbladder
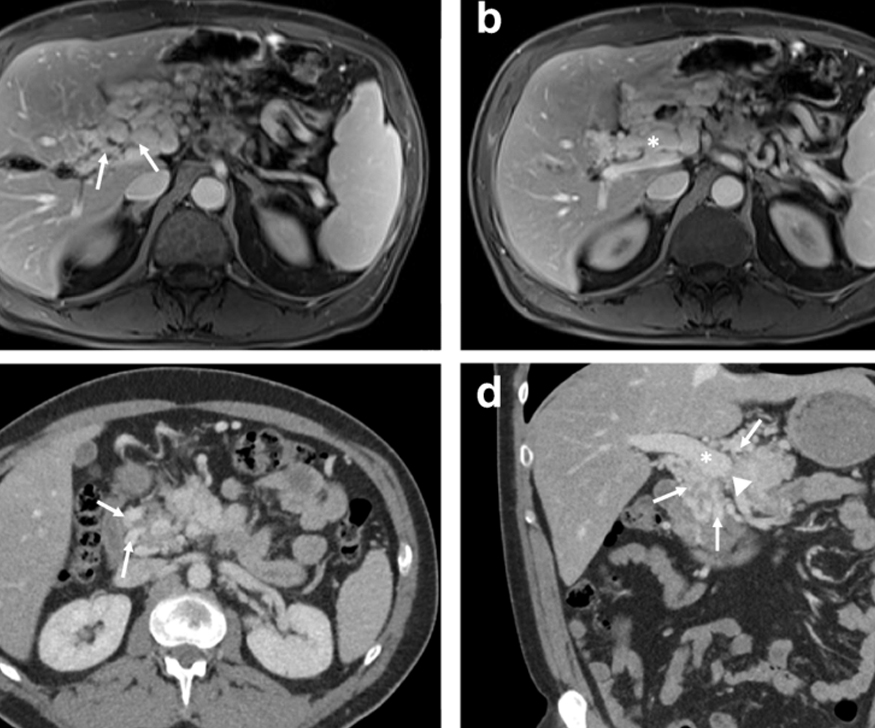
CECT scan showing duplication of the gallbladder
Discussion
Gallbladder duplication is a rare congenital anomaly with an incidence of 1 in 3000-4000. According to Boyden’s classification, it can be classified into two main types:
(i) Vesica fellea divisa (bilobed or bifid gallbladder)
(ii) Vesica fellea duplex (double gallbladder with two cystic ducts), which may be Y-shaped (united before entering the common bile duct) or H-shaped (two cystic ducts entering separately into the biliary tree).
It is important that the condition be diagnosed preoperatively as the second gallbladder may either be overlooked during surgery or pose an increased risk of injury to the biliary tree. Ultrasonography is the preferred first line of imaging. However, several other pathologies may mimic a duplicate gallbladder on ultrasonography viz. folded gallbladder, choledochal cyst, phrygian cap, pericholecystic fluid, gallbladder diverticulum, vascular band across the gallbladder and focal adenomyomatosis.
MRCP is the subsequent investigation of choice, not only to rule out the above, but more importantly to evaluate the biliary tree, particularly the cystic duct. CECT is also a simple but useful modality of investigation. Laparoscopic
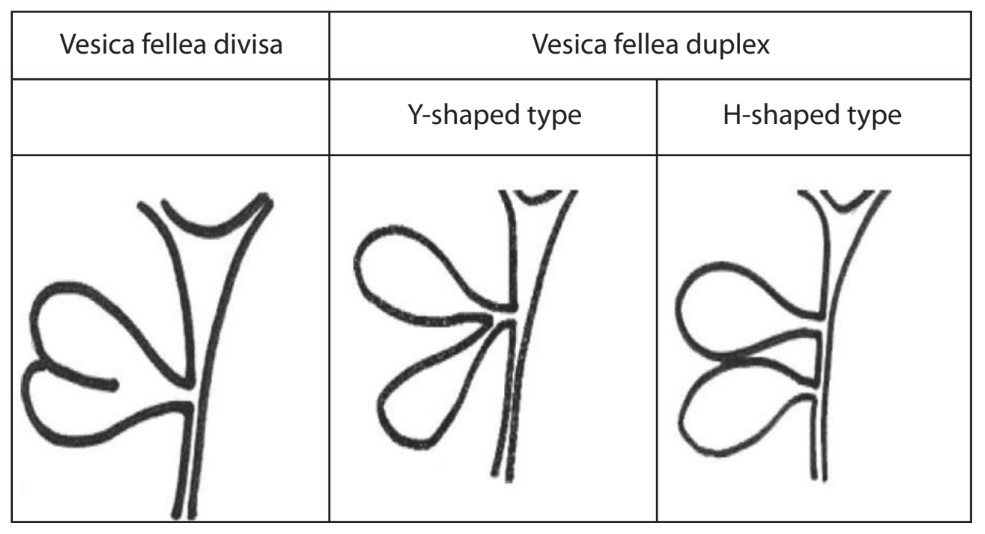
Boyden’s Classification
Dr. Susenjit Prasad Mahato, one of the best gallbladder surgeon in kolkata, has operated many critical gallbladder surgeries successfully with his great experience and efficiency. This rare case was one of his biggest challenge which also had been operated successfully.